How do you market the scariest product in healthcare?
A go-to-market teardown of Hippocratic AI — and the plan I’d run next.
A teardown by Aline Aronsky. I spent two years running go-to-market for enterprise clinical software; here’s how I read the fastest-moving company in healthcare AI.
The bet
Hippocratic’s safety claim isn’t a slogan a rival can borrow — it’s three years of compounding proof: validated interactions, a clinician network, a zero-incident record nobody else can backdate. That’s a real moat. What’s imitable is the word “safe,” not the asset behind it — and right now Hippocratic is spending that asset on the wrong audience. The proof stack reassures the clinician in the room. It should be doing the harder job: arming the champion who has to leave the room and defend this purchase to a boss who wasn’t.
Within 90 days, repackage the existing proof stack as a “make the case to your boss” toolkit and track champion-to-approval velocity — the days between a champion first raising Hippocratic internally and getting sign-off. If usage goes up but velocity doesn’t move, I’m wrong that internal buy-in — not clinical trust — is the binding constraint.
The category, in one screen
For the reader who doesn’t live in healthcare.
Healthcare AI agents are voice AIs that talk to patients directly — calling to check in after surgery, walking a chronic-disease patient through their meds, running pre-visit intake. Not chatbots on a website; autonomous agents on the phone, at scale.
Why now: US healthcare is short hundreds of thousands of nurses, and the work that burns them out most is high-volume, repetitive, non-diagnostic outreach — exactly what a voice agent can do. Generative AI got good enough to hold these conversations around 2023; by 2026 the category has minted multiple unicorns. Hippocratic reached a $3.5B valuation in roughly 15 months of selling.
The catch — and the entire marketing problem — is that people are scared of AI touching patient care. So this category isn’t sold on features. It’s sold on trust.
Subject snapshot
The teardown
Five GTM dimensions — the diligence behind the bet.
Positioning & messaging
Hippocratic runs a one-word strategy: safety. The claims are superlative and validation-anchored. The sharpest move: the guardrail list reads as a legal disclaimer but functions as the core trust pitch — they turned “what we refuse to do” into the reason to believe.
“Safest Healthcare Generative AI Agents”
“Do no harm.”
“We do not diagnose or prescribe… do not handle mental health disorders.”
hippocraticai.com · CTA: “Book a Meeting” (no pricing, no self-serve)
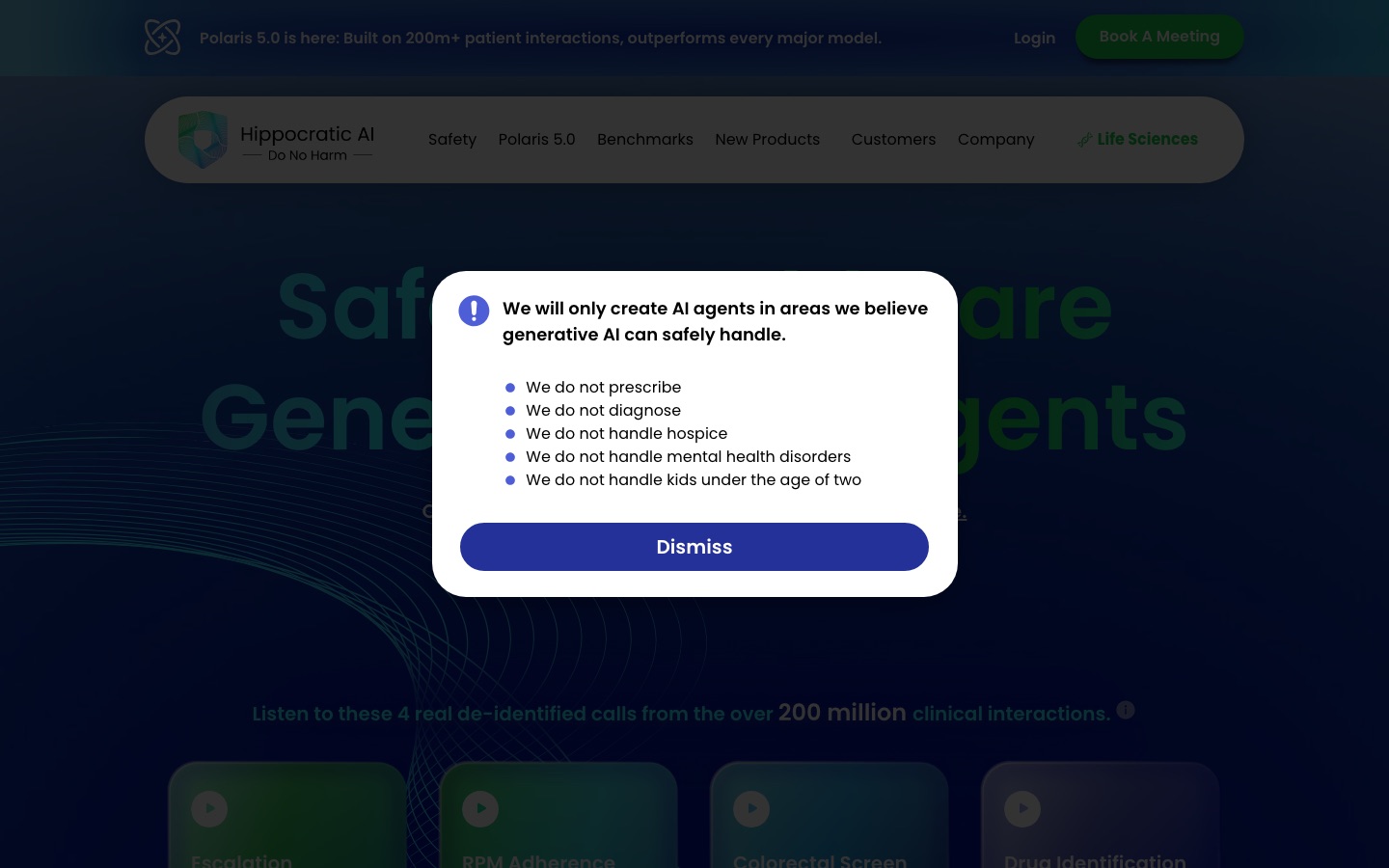
Everything signals enterprise, sales-led, trust-first. The guardrails aren’t caveats — they’re the pitch.
ICP & the wedge
The category label they coined — “Super Staffing” — is positioning as objection-handling: multiply clinician capacity, don’t replace it. That single frame defuses the clinician-fear objection before it’s raised. The wedge use cases (post-discharge calls, chronic-care check-ins, pre-op screening) are the lowest-liability, highest-volume slice of clinical work — also the safest place to prove the safety claim.
Investors who are also customers who are also reference logos — UHS, Cincinnati Children’s, WellSpan.
The trust play Standout
The category’s central question is “how do you sell a product people are afraid of?” Hippocratic’s answer: drown the fear in third-party-validated numbers and visible constraint. Every trust claim is either a countable proof or an external validator. Even the model architecture is sold as a safety feature. And the human touch — WellSpan naming its agent “Anna” — quietly reframes “scary AI” as “a colleague.”
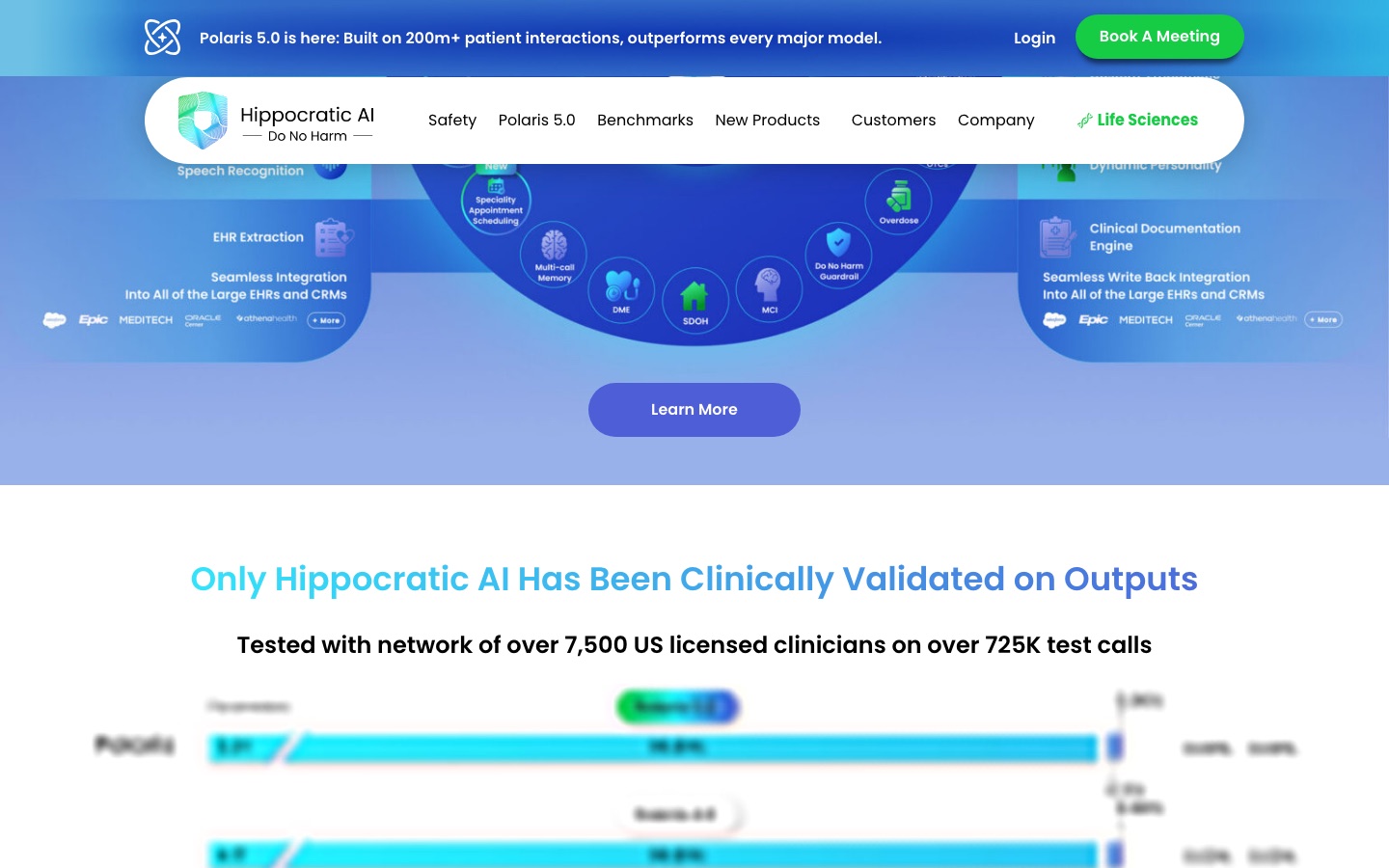
7,500 licensed clinicians · 725K test calls
115M+ patient interactions · zero safety incidents
HIPAA · SOC 2 · “Only Hippocratic has been clinically validated on outputs”
Selling into health systems, the objection I hit most often wasn’t clinical — it was political. The person across the table wasn’t asking “is this safe enough for my patients.” They were asking, in effect, “how do I convince my boss?” That’s a different question, and it needs a different piece of ammunition than a trust badge aimed at a clinician’s fear. The durable part of Hippocratic’s moat isn’t the word “safe” — it’s that nobody else has three years of compounding, third-party-validated proof to hand a nervous champion. The imitable part is the marketing choice to spend all of it reassuring the room, instead of arming the person who has to leave the room and sell it upstairs.
Channel & motion
Three moves worth dissecting. Borrowed credibility — the NVIDIA partnership pairs a scary product with the most trusted name in AI (deployed on AWS for enterprise comfort). The App Store — clinicians build, validate, and share revenue on agents, turning customers into a distribution flywheel. And PR set-pieces that make abstract capability sympathetic:
“100,000 patient calls in a single day during a Florida hurricane.”
Converts “AI replacing nurses” into “AI showing up when humans couldn’t.”
Founder-led thought leadership (Shah’s interview/podcast circuit) is a primary channel, not a side activity.
Pricing & packaging
Pricing isn’t on the site — but the reported anchor is the sharpest thing in their whole GTM:
~$9 per agent-hour vs. ~$45/hour for a nurse.
Reported (press/analyst), not an official pricing page — flagged as such.
That one comparison reframes a frightening purchase as obvious labor arbitrage — moving the buyer from “is this safe?” to “can I afford not to?” The striking part: it’s buried behind a meeting request instead of leading the story.
The field
Hippocratic is the only one who planted a flag in “clinical.”
The open question: is that flag a moat — or just a head start?
What’s working — and the whitespace
Four openings. The teardown’s job is to pick a fight, not list options.
The safety moat is loud but imitable.
Winning the word “safe” first is real — defensible only if it compounds into something copiers can’t match. Otherwise it’s everyone’s tagline by 2027.
Fear is handled; desire is not.
Nearly all messaging answers “is it safe?” Little answers “what do I gain?” — burnout relief, capacity, revenue recovered. An outcome/ROI narrative sits unbuilt on top of the safety floor.
The $9 anchor is under-deployed.
Their single best line is behind a “Book a Meeting” wall.
Buyer sprawl.
“Providers, payors, and pharma” + “1,000+ agents” risks a horizontal story. Naming one hero outcome — readmissions, with its P&L — would sharpen everything.
Two of these I’d stake a plan on. The safety moat is real, not imitable — every call logged and every incident-free month is a data point a rival can’t backfill by copying a tagline. But Hippocratic is running it like a slogan instead of proving it’s structural, so it reads imitable even though it isn’t. Fix: show the curve, not just the count. And fear is handled, desire isn’t — that gap is exactly where deals stall, because the clinician’s reassured but nobody’s armed the person who has to defend the purchase to their own boss. Fix both and a trust badge becomes a sales weapon.
The 90-day plan
If I were on Hippocratic’s marketing team — my first 90 days. This is the page that gets the interview.
Built, not just graded
Example builds — a critic describes; an operator ships. Replace these with your own; the making is the point.
“Safest Healthcare Generative AI Agents”
“The 30% fewer readmissions your nurses don’t have time to chase.”
“Safest Healthcare Generative AI Agents”
“The proof your boss needs before you can say yes.”
Two different shifts, same floor. The first moves fear → desire (safety → an outcome). The second moves audience — from reassuring the clinician in the room to arming the person who has to sell it to someone who isn’t.
“$9 vs $45.” Labor-arbitrage campaign for CFOs. Visual: a shift schedule that fills itself.
“Meet Anna.” Humanize the agent (borrow WellSpan’s naming) to disarm clinician fear. Testimonial-led.
“When the hurricane hit.” The 100K-calls story as a brand film about showing up.
| Audience | Their fear | The desire we sell | Proof we lead with |
|---|---|---|---|
| CFO | wasted spend / risk | $9-vs-$45 labor math | ROI calc · 30% readmit ↓ |
| CNO / nursing | “replacing my nurses” | capacity + burnout relief | “Super Staffing” · Anna |
| Compliance / legal | patient-safety liability | validated, constrained AI | 0 incidents · HIPAA / SOC 2 |
| Champion / internal sponsor | looking exposed for backing this | a credible case pre-built to hand upward | the internal-approval toolkit — ROI math + validation curve + peer references, ready to forward |